 Fractures of the distal radius are the most common injury of the wrist. This injury can result from mild impact such as a fall onto the out-stretched hand through to high energy injuries such as mountain bike & motor vehicle accidents. In older patients a fracture of the writs may be a sign of osteoporosis and a bone density test should be performed after the fracture has been treated.
Fractures of the distal radius are the most common injury of the wrist. This injury can result from mild impact such as a fall onto the out-stretched hand through to high energy injuries such as mountain bike & motor vehicle accidents. In older patients a fracture of the writs may be a sign of osteoporosis and a bone density test should be performed after the fracture has been treated.
The wrist is made up of the two long bones of the forearm, the radius and ulnar, and the eight small bones of the wrist.
The severity of the force usually corresponds to the degree of damage. Higher impact injuries cause more severe fractures and joint damage.



 Extra-articular – does not involve the joint
Extra-articular – does not involve the joint
Intra-articular – involves the joint
Non-displaced – there is a fracture, but the bone has not moved out of position
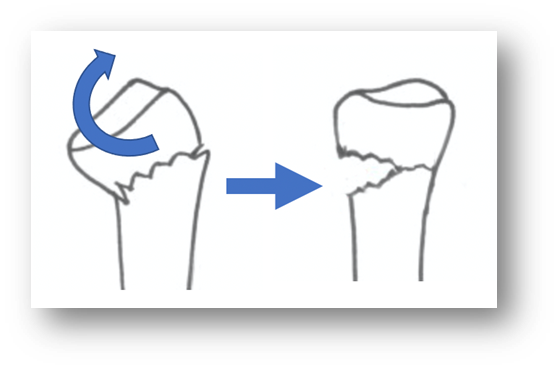
Displaced – the fracture has moved out of position
Angulated – bent at an angle
Comminuted – in many pieces



 Open Reduction & Internal Fixation (ORIF)
Open Reduction & Internal Fixation (ORIF)
Colle’s and other distal radius fractures that are displaced, angulated, or comminuted will usually be treated by “open reduction and internal fixation (ORIF)”. This involves a general anaesthetic and a 60–90-minute operation where an ~10cm incision is made on the forearm and a plate and screws are inserted once the fracture has been “reduced” (put back in its normal position or close to it). X-rays are taken in the operating theatre to check the fracture and plate position. Most people prefer to stay overnight for pain relief, but this is not essential